
Ask any mental health clinician what their least favorite part of the job is, and documentation will probably come up.
Take treatment planning. It’s meant to be a collaborative, personalized roadmap for care. But it’s also a billing requirement. So we’re stuck walking a tightrope—trying to write something that’s clinically meaningful, audit-proof and won’t take us our entire lunch break to write. With no real standard, most of us are left guessing.
Is this plan compliant? Did I show medical necessity? Will this justify continued care if a payer audits? Is it actually useful—or just something I rushed through between sessions?
If that sounds familiar, you’re not alone. We’ve found most clinicians (ourselves included) fall into one of three camps:
Writing super long plans to try and cover every base
Writing short, copy-paste plans and hoping no one looks too closely
Writing clinically helpful plans… that are somehow non-compliant
And it’s hardly surprising. Treatment plans aren’t tied to CPT codes, you don’t get reimbursed for writing them. But if your plan doesn’t meet insurance standards? They can deny claims—or worse, ask for repayment for every session linked to that plan. All whilst providing very little actionable guidance on what compliance means.
To make things harder, treatment plans are usually written after a few sessions. By then, you’re piecing together scraps from around the chart and trying to remember what your client actually said their goals were last week.
And while EHRs can help with structure, most rely on generic templates that don’t reflect how you actually work—and definitely don’t guarantee compliance.
That said, a solid treatment plan can be invaluable:
Offering a rich biopsychosocial understanding of your client
Strengthening the therapeutic alliance
Supporting high quality decision-making by tracking goals, progress, and treatment rationale
Over the past 6 months, I’ve been digging into what makes a treatment plan both clinically meaningful and compliant—without eating up your evening.
This guide walks you through each section step-by-step, explains why it matters, and includes a plug-and-play template you can start using right away.
Session Data
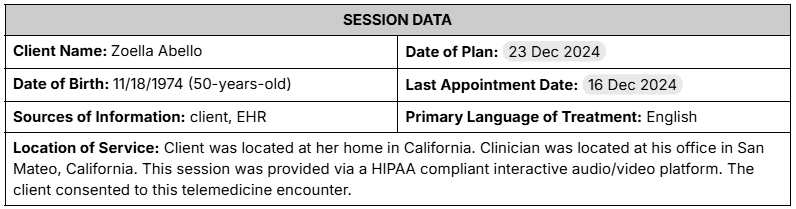
The template begins with administrative information necessary for filing. Unlike a progress note, it is not necessary to document the time or length of the appointment. For telehealth appointments, the note should include the location of both the clinician and patient, attest to the use of a HIPAA compliant telehealth platform, and note your client’s consent to use of telehealth. For in-person appointments, note only the location of the office in which the appointment took place. It is required that the clinician be licensed to practice in the state where the client is located.
Clinical Context

This heading highlights your client’s challenges that are being addressed in treatment.
The Chief Complaint captures the primary reason your client decided to seek care.
Core Problems summarize your client’s greatest areas of difficulty and may include psychiatric and general medical problems, social challenges such as unemployment and isolation, addictive behaviors, legal problems, and other relevant stressors. These statements should include related symptoms and behaviors that illustrate the problem. Language should be non-judgmental and non-technical as this plan may be read by your client and their significant others. Your client may have more than three categories of identified problems, but it is usually best to focus on those with the highest priority.
Biopsychosocial History
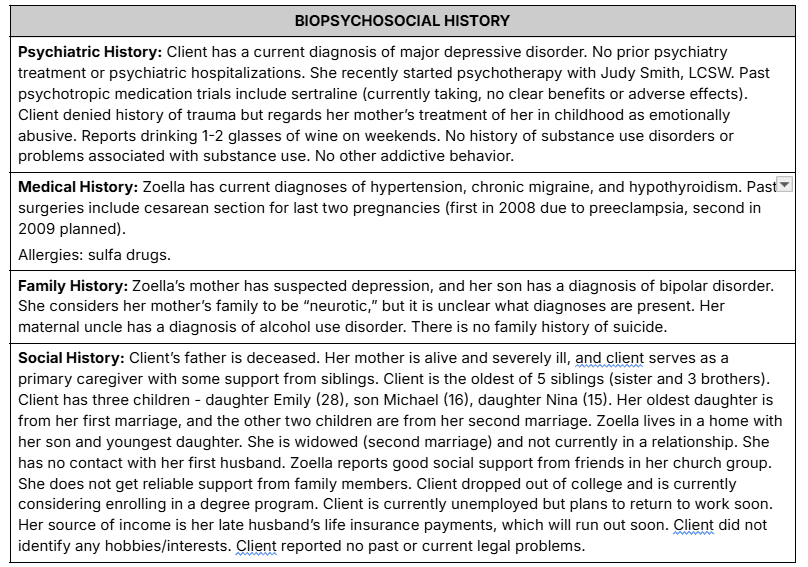
This heading summarizes your client’s biological, psychological, and social context. These summaries need not be exhaustive; include only information pertinent to conceptualizing your client’s experience.
Common details included in each section include:
Psychiatric History: current and past psychiatric diagnoses, previous psychiatric evaluations, history of psychiatric outpatient treatment, psychiatric hospitalizations, PHP/IOP admissions, current and past treatment with psychotherapy and psychotropic medications, history of substance abuse/misuse and addictive behaviors
General Medical History: general medical diagnoses, active treatment for medical conditions, past surgeries, allergies
Family History: family psychiatric history, family history of addiction, family history of suicide
Social History: home environment, family structure, relationships and friendships, social support systems, education, occupational history, interests and hobbies, religion and faith, legal history
Strengths and Risks
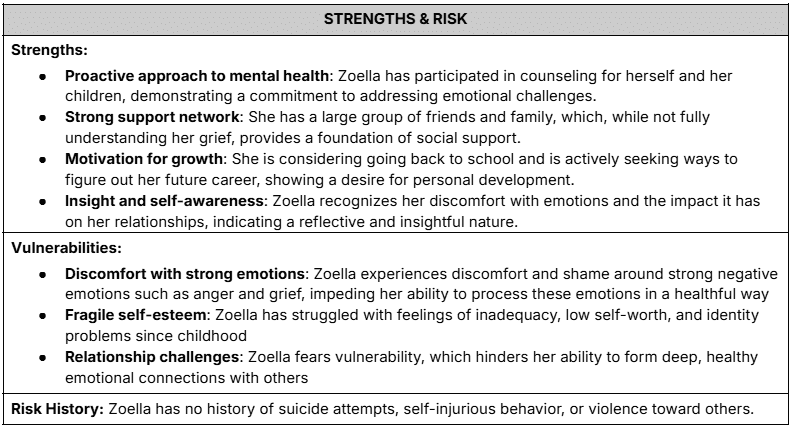
This heading summarises strengths and vulnerabilities that should be considered in your client’s treatment journey.
Strengths are notable skills, attributes, or resources that can be leveraged to help them progress toward their goals. This can include evidence-based resilience factors and other notable positive features identified by the clinician.
Vulnerabilities are attributes that could potentially impede the therapeutic process or lead to regression if not accounted for. This can include evidence-based risk factors and other pervasive areas of difficulty.
As past unsafe behavior is the strongest predictor of future unsafe behavior, it can be useful to record your client’s personal history of self-injury, suicide attempts, or aggression toward others, or the lack thereof.
Goals and Progress
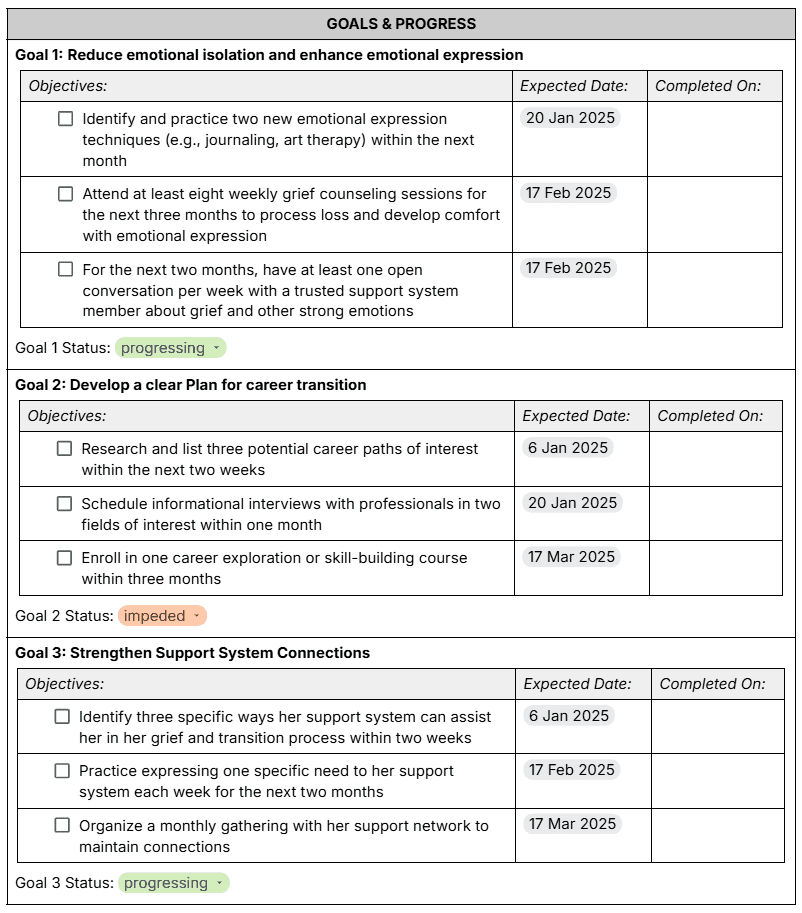
Recording and tracking treatment goals is one of the most unique aspects of treatment plans, compared with other documentation. Goals and objectives should be determined collaboratively, with both the clinician and client agreeing on what is included in the plan.
Goals are the big-picture outcomes your client wants to achieve as a result of treatment. They are often directly tied to core problems (outlined earlier in the plan). The best goals are clear, specific, and reasonable for the client’s current circumstances. Stick to 1-3 goals to keep the treatment focused. You can always modify them at future reviews.
Objectives are the steps a client will take to accomplish their identified goals. The best objectives follow the SMART format:
Specific - clinician and client can easily understand the objective
Measurable - progress toward the objective can be simply evaluated.
Attainable - the objective is realistic, given the client’s circumstances and stage of care
Relevant - the objective is aligned with the client’s values and wider goals
Time-Limited - the objective specifies a time frame for completion
The template includes a menu to note the status of the goal, providing a succinct evaluation of progress.
Summary of Treatment Recommendations

This heading lists the client’s active treatments recommendations.
The first subsection lists the members of the client’s care team such as physicians, therapists, and coaches and what services they are providing. It can be helpful to know who is accountable for which aspects of treatment.
The next subsections list active medications and psychotherapies, the cornerstones of most mental mental healthcare plans. Charts are included to help record important details of these interventions and track your client’s response to them.
Lastly, it is important to record other recommendations intended to support the client in achieving their goals. This may include social, environmental, or behavioral recommendations such as changes in habits or wellness activities.
Footer
The footer of the Treatment Plan notes the date of the next time the plan will be reviewed with the client, allowing for modifications and progress tracking. Treatment plans should always be reviewed by the client and signed by both the clinician and client.
A note on AI-friendly formatting
Emerging AI applications are rapidly changing clinical workflows. In designing a template from the ground up, I wanted to make sure it allows clinicians to take full advantage of these tools. I used free text, narrative formatting where possible to allow for smooth integration of generative AI outputs.
Checklist
While there are no standard requirements for a mental health Treatment Plan, this checklist should ensure satisfy compliance requirements in almost every case:
|
Conclusion
In this post, we have discussed the challenges clinicians face with treatment plan documentation and explored a framework for creating high-impact plans. You can find a blank copy of my treatment plan template at this link.
Let us know what has worked for you in your treatment plans—we’re always improving.
Try Allia for yourself
Getting started with Allia takes less time than making your morning coffee:
Create your free account - no payment info, no fine print.
Set up your practice details.
Jump straight into telehealth, notes, and billing tools that just… work.
That’s it. No hoops to jump through, no catch waiting around the corner.
If you’d like to see what a fully functional, truly free EHR with AI support can feel like, you can create your Allia account today. No restrictions, no hidden add-ons.
Want to see how it works? Sign up for Allia today.


